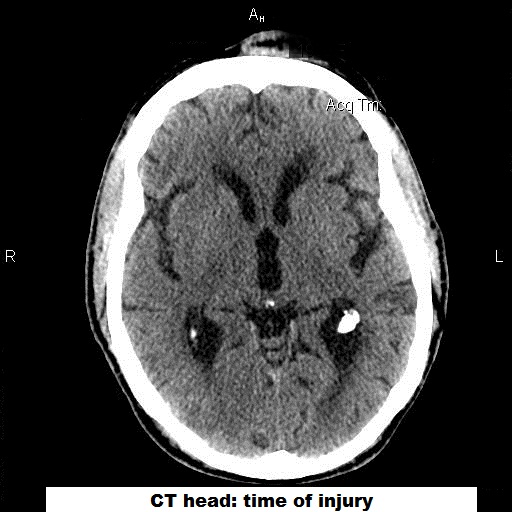
An 83 y/o man was out for a daily walk in his neighborhood when he was discovered by a passerby to be face-down bleeding from his nose. He was rushed to the local ED where he was confused and complaining of pain at multiple sites. After extensive tests, the only pertinent abnormality was a small bleed in the lateral ventricle of the right frontal lobe of his brain. Once returned to home and healed from his minor bruises and strains, it was clear to his family that there had been a change to this patient both physically and emotionally. He no longer walked confidently and now exhibited small cautious steps. For the first time in his life, he began having problems with urinary urgency in which he would have to hurry to the bathroom in order to urinate. At night he began wearing adult diapers. He also became more confused and had to be looked after by his wife. In essence, he regressed to being more like a toddler. His wife had to assume more of the daily household activities. He stopped driving.
On exam, the most striking feature was a slow, cautious gait with difficulty turning around. Otherwise the exam was non-focal.
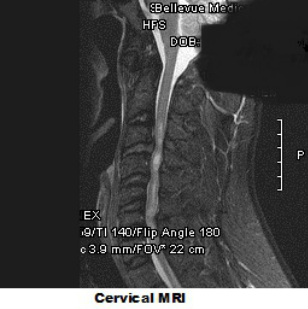
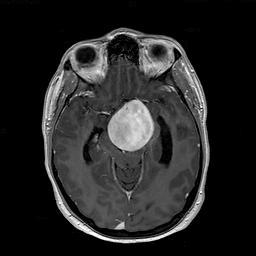
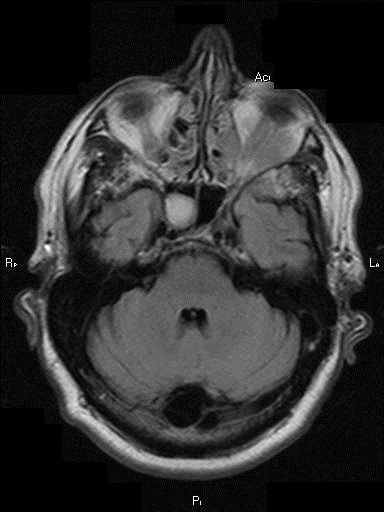
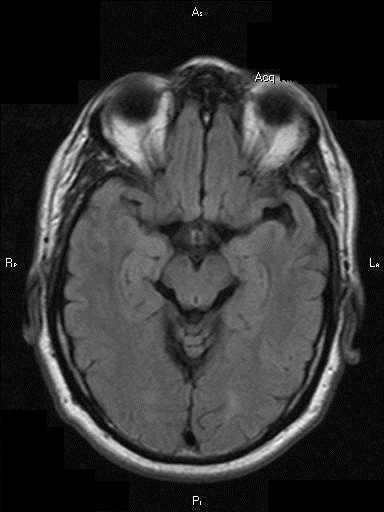
First, an MRI of the brain showed signs that cerebrospinal fluid (CSF) was pushing into the adjacent brain (‘transependymal flow’). In addition, when comparing the size of the ventricles (the chambers found in the center of the brain that house the CSF) to the size of the ventricles from a pre-accident MRI, it was clear that the ventricles were much larger. This suggested that he had acquired hydrocephalus (‘water on the brain’).
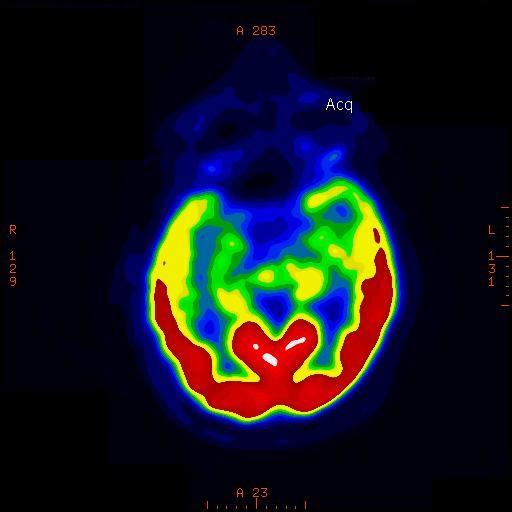
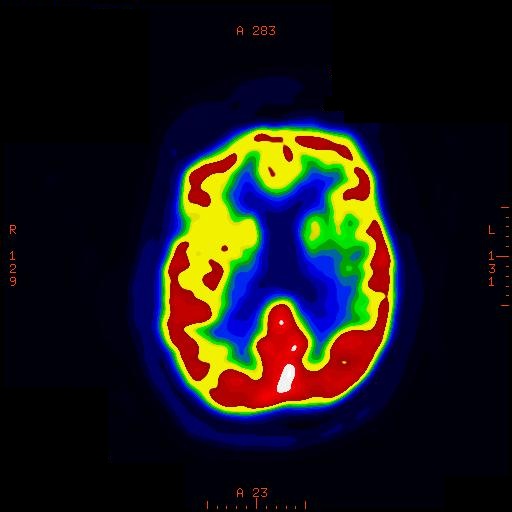
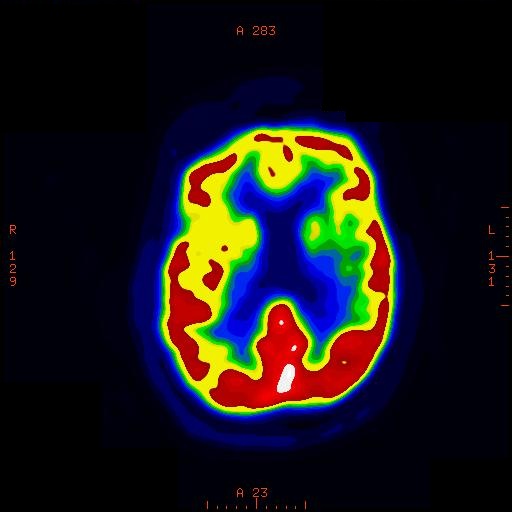
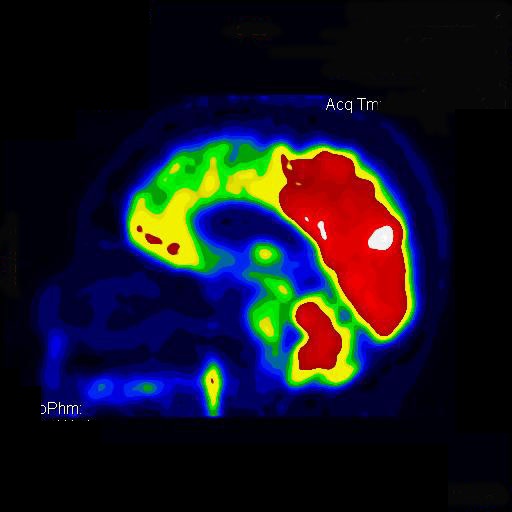
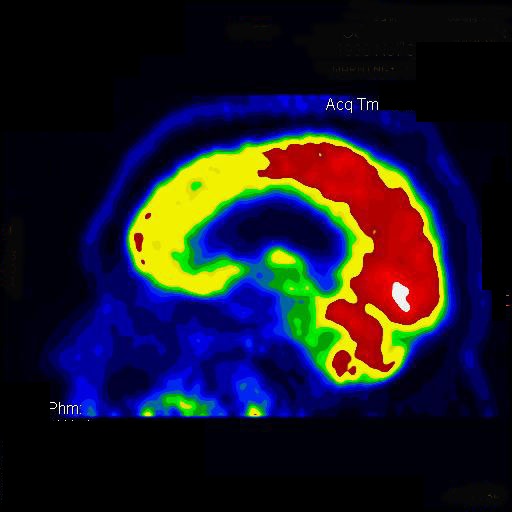
I then sent him for a lumbar puncture which revealed a normal pressure when performed – rather than an elevated pressure as one might expect. I then performed a nuclear study called an Indium-111 cisternogram in which radioactive Indium-111 is injected into the CSF around the lumbar spinal cord. In a normal person, this Indium-111 will not collect inside the ventricles but with patients who have a condition called Normal Pressure Hydrocephalus (NPH), the Indium-111 does end up inside the lateral ventricles. This test was positive for this patient.
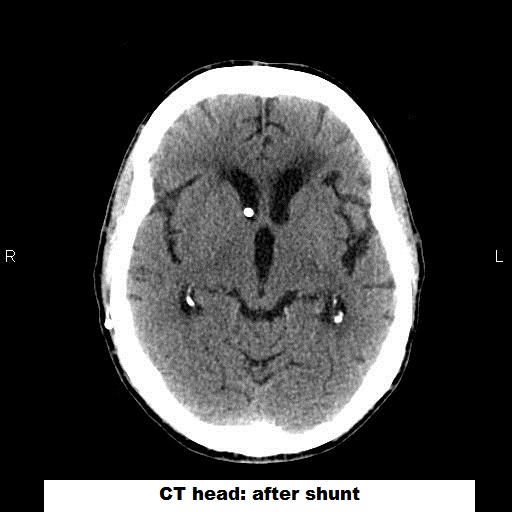
He underwent placement of a ventriculoperitoneal (VP) shunt and immediately showed a return to his normal walking pattern and had resolution of his urinary urgency. The confusion improved as well.
First, an MRI of the brain showed signs that cerebrospinal fluid (CSF) was pushing into the adjacent brain (‘transependymal flow’). In addition, when comparing the size of the ventricles (the chambers found in the center of the brain that house the CSF) to the size of the ventricles from a pre-accident MRI, it was clear that the ventricles were much larger. This suggested that he had acquired hydrocephalus (‘water on the brain’).
I then sent him for a lumbar puncture which revealed a normal pressure when performed – rather than an elevated pressure as one might expect. I then performed a nuclear study called an Indium-111 cisternogram in which radioactive Indium-111 is injected into the CSF around the lumbar spinal cord. In a normal person, this Indium-111 will not collect inside the ventricles but with patients who have a condition called Normal Pressure Hydrocephalus (NPH), the Indium-111 does end up inside the lateral ventricles. This test was positive for this patient.
He underwent placement of a ventriculoperitoneal (VP) shunt and immediately showed a return to his normal walking pattern and had resolution of his urinary urgency. The confusion improved as well.

DIAGNOSIS: NPH
Normal Pressure Hydrocephalus is thought to occur as a result of blockage of arachnoid granulations by degraded blood products. Normally, the arachnoid granulations are responsible for resorption of the used CSF. If an individual has experienced an intracranial bleed then they are theoretically at risk for developing NPH afterwards. The classic clinical triad is ‘wild, wet and wobbly’ meaning worsening cognition, change in urinary habits and change in gait. The treatment is placement of a VP shunt which will drain a small amount of the CSF continuously into the person’s gut.
Normal Pressure Hydrocephalus is thought to occur as a result of blockage of arachnoid granulations by degraded blood products. Normally, the arachnoid granulations are responsible for resorption of the used CSF. If an individual has experienced an intracranial bleed then they are theoretically at risk for developing NPH afterwards. The classic clinical triad is ‘wild, wet and wobbly’ meaning worsening cognition, change in urinary habits and change in gait. The treatment is placement of a VP shunt which will drain a small amount of the CSF continuously into the person’s gut.




 RSS Feed
RSS Feed
